Proximal tibia volumetric bone mineral density is correlated to the magnitude of local acceleration in male long distance runners.
"Male runners present generally higher BMD than sedentary individuals. We postulated that the proximal tibia BMD is related to the running distance as well as to the magnitude of the shocks (while running) in male runners."
Running at minimum causes trabecular microfractures and increases bone mineral content. The theory was that the amount of microfractures caused is related to the force of impact generated while running and the duration of exercise.
"Several measurements were performed at the proximal tibia level: volumetric BMD (vBMD), cortical index (CI) i.e. an index of cortical bone thickness and peak accelerations (an index of shocks during heel strike) while running (measured by a 3-D accelerometer)."
The cortical index could be very useful to us as a measurement tool to determine when cortical microfractures have occurred.
"CI and vBMD a) increase with running distance to reach a plateau over 30 km/wk, b) are positively associated with peak accelerations over 30 km/week."
"CI and vBMD are associated with the magnitude of the shocks during heel strike in runners."
The faster you run and the harder you strike the ground the more microfractures you cause. The fact that cortical index leveled off over time goes against our microfracture theory. As you should always be able to cause microfractures(unless there's a performance issue where you're not able to run as hard or fast or there's an adaptation issue where over time the same impact no longer causes cortical microfractures). Perhaps the cause of the increase in cortical bone size is by other factors than microfracture healing.
Note however that the sedentary individuals are actually the tallest and that the more the individuals ran per week the shorter they tended to be. This could be due to proteoglycan depletion and other factors from articular cartilage. It could also be due to shorter individuals enjoying going running more. There would have to be a longitudinal study done to know the true effect of running on height.
Bone mass and geometry of the tibia and the radius of master sprinters, middle and long distance runners, race-walkers and sedentary control participants: a pQCT study.
Note in this study the control group also tended to be taller than the runners but there was seemingly no correlation between height and distance ran like in the other study.
"As hypothesised, tibia diaphyseal bone mineral content (vBMC), cortical area and polar moment of resistance were largest in sprinters, followed in descending order by middle and long distance runners, race-walkers and controls. When compared to control people, the differences in these measures were always >13% in male and >23% in female sprinters (p<0.001)."
Diaphysis is the midshaft section of the bone. The healing of microfractures induced by running would increase bone mineral content in that area. The use of the terminology cortical area rather than cortical volume alludes to the fact their was no increase in height.
"Similarly, the periosteal circumference in the tibia shaft was larger in male and female sprinters by 4% and 8%, respectively, compared to controls (p<0.001)."
Sprinting creates a strong enough chemical and mechanical signaling to increase periosteal width. Periosteal width is different from the deposition of new bone beneath the periosteum.
"Epiphyseal group differences were predominantly found for trabecular vBMC in both male and female sprinters, who had 15% and 18% larger values, respectively, than controls (p<0.001)."
So trabecular microfractures were caused first, followed by cortical microfractures, and followed by an increase in periosteal width.
This study did not take place over a duration of time so it could not have studied a change in bone length.
What we learned though is that sprinting is sufficient to cause cortical microfractures by the fact that cortical area increased. There's no basis as to why if cortical length and width can increase that cortical height can't increase as well(unless sprinting causes microfractures in a way that only results in an increase of length or width of the bone when the microfractures are healed). However, there doesn't tend to be cortical bone in the epiphysis. The reason why periosteal width can increase with some stimulus and the epiphysis can't is that they are different tissues. To increase the height of the epiphysis requires special stimulation. The healing mechanisms for bone differ from how the cortical bone is aligned as cortical bone tends to increase in width rather than height(likely due to the OPG/RANKL gradient).
Note that the long distance runners had the greatest epiphyseal area. This could however be due to less modeling into cortical bone.
Growth and adaptation to mechanical loading of immature bone and articular cartilage
"The osteogenic response due to different running modes was greatest in the femoral metaphysis. In particular, solely downhill running with high proportions of eccentric loadings was able to increase femoral trabecular bone mineral density in the metaphysis, while level running with similar amounts of concentric and eccentric loadings failed to induce an osteogenic response in this area. In contrast, neither in the dia- nor in the epiphysis any running mode-related structural alteration could be found. Moreover, downhill running increased femoral cartilage height and COMP staining height in a site-specific manner, while level running was insufficient to induce such alterations. These changes were not accompanied by any signs of degeneration. In contrast, cartilage thickness, mechanical properties, and expression of major cartilage network proteins (i.e., collagen II, collagen IX, COMP, and matrilin-3) in tibial cartilage remained unaffected by the different running modes. Growth was associated with high modeling of the morphology, biochemical composition, mechanical properties of articular cartilage, and structure of subchondral bone. COMP showed a profound redistribution throughout the cartilage. Moreover, growth diminished cartilage thickness, distribution and amounts of the matrix proteins collagen II, collagen IX, and matrilin-3 and related to this decreased its compressive properties. Functional condensation of the subchondral trabecular bone and subchondral plate due to enchondral ossification was also found to occur with increasing age, which did not seem to affect cartilage mechanical properties. In conclusion, these are the first in vivo data illustrating the effect of different running modes with different proportions of eccentric and concentric loadings on immature bone and articular cartilage in such a physiological and systematic manner."
This study was in a foreign language and I could not get the full thesis.
HEre's the running study though:
"Mechanical loading plays an important role not solely in cartilage development, but also in cartilage degeneration. Its adaptation behavior to mechanical loading has not been clearly delineated. The aim of the study was to examine the effect of different running modes (with different muscle contraction types) on morphological, biochemical, and mechanical properties of articular cartilage in the knee of growing rats. Thirty-six female Sprague-Dawley rats were randomly assigned into a nonactive age-matched control (AMC), level (LEVEL), and 20° downhill (DOWN) running group (n = 12 each). Running groups were trained on a treadmill for 30 min/day, 5 days/week for 6 weeks. Immunohistochemical staining and analysis of expression for collagen II, collagen IX, cartilage oligomeric matrix protein (COMP), and matrilin-3, histomorphometry of femoral cartilage height and femoral COMP staining height, and indentation testing of tibial articular cartilage were performed. Rats subjected to downhill running showed a significantly (P = 0.015) higher COMP staining height and a tendentially (P = 0.084) higher cartilage height in the high-weight bearing area of femoral articular cartilage. Cartilage thickness, mechanical properties, and expression of cartilage network proteins in tibial cartilage remained unaffected by different running modes. Our data suggest that joint loading induced by eccentric muscle contractions during downhill running may lead to a site-specific adaptation."
couldn't get full study
couldn't get full study
Here's a study linking muscular contractions to articular cartilage deformation.
There is actually mixed data on whether running is anabolic:
"Cartilage loading is associated with the onset and progression of osteoarthritis and cell death may play an important role in these processes. Although much is known about cell death in joint impact loading, there is no information on joints loaded by muscular contractions. The aim of this study was to evaluate the influence of muscle generated eccentric and concentric submaximal joint loading on chondrocyte viability. We hypothesised that eccentric muscle activation leads to increased cell death rates compared to concentric loading and to controls. 16 rabbits received either 50 min of uni-lateral, cyclic eccentric (n=8) or concentric (n=8) knee loading. Muscle activation for these dynamic conditions was equivalent to an activation level that produced 20% of maximum isometric force. Contralateral joints served as unloaded controls. Cell viability was assessed using confocal microscopy. Eccentric contractions produced greater knee loading than concentric contractions. Sub-maximal contractions caused a significant increase in cell death in the loaded knees compared to the unloaded controls, and eccentric loading caused significantly more cell death than concentric loading. Cyclic sub-maximal muscle loading of the knee caused increased chondrocyte death in rabbits. These findings suggest that low levels of joint loading for prolonged periods, as occurs in endurance exercise or physical labour, may cause chondrocyte death, thereby predisposing joints to degeneration."
It's unclear why this study got a catabolic result and the other one didn't. They did measure different things. Couldn't get full study.
"Mice were divided into five groups: sedentary (SED), uphill training (TRU), downhill training (TRD), excessive uphill training (ETU), and excessive downhill training (ETD) for an 8-week training intervention protocol.
ETD group had increased pro-inflammatory cytokines in serum, vastus lateralis (VL), and vastus medialis (VM) muscles, while ETU group mice had increased cytokine levels in the VL and VM. Total knee joint OARSI score were more significant in ETD group compared to SED and TRU groups. They were also more meaningful for the medial tibial plateau of ETD group compared to SED group. MMP-3 and cleaved Caspase-3 were higher in the ETD group than the SED and TRU group, while Adamts-5 was higher in the ETD group than the SED group. TRU group had increased PRG-4 levels compared to ETU and ETD group. ETD group had decreased total bone volume, trabecular bone volume, and cortical thickness compared to SED group.
Excessive downhill training induced a chronic pro-inflammatory state in mice and was associated with early signs of cartilage and bone degeneration that are clinical indicators of knee OA."
Key term is excessive.
"Increased levels of IL-1beta have been observed in OA cartilage, and high serum levels of IL-6 and TNF-alpha have been associated with cartilage loss. Moreover, IL-1beta promotes the release of MMP-3 (Matrix Metalloproteinase-3) and the aggrecanase Adamts-5 (a disintegrin and metalloproteinase with thrombospondin motifs-5), enzymes involved in articular cartilage matrix degradation, a hallmark of OA. Also, metabolic inflammation has been related to increased chondrocyte apoptosis. In contrast, PRG-4 (Proteoglycan 4/Lubricin) reduces friction between biological surfaces promoting tissue homeostasis"
Here's the articular cartilage:

Uphill and downhill training looks like it has thicker cartilage than controls but I can't tell.
"High joint loads can trigger bone remodeling"
Long-term repetitive mechanical loading of the knee joint by in vivo muscle stimulation accelerates cartilage degeneration and increases chondrocyte death in a rabbit model
"24 rabbits were divided into an (i) eccentric, (ii) concentric, or (iii) isometric knee extensor contraction group (50 min of cyclic, submaximal stimulation 3 times/week for four weeks=19,500 cycles) controlled by the stimulation of a femoral nerve cuff electrode on the right hind limb. The contralateral knee was used as a non-loaded control. The knee articular cartilages were analysed by confocal microscopy for chondrocyte death, and histologically for Mankin Score, cartilage thickness and cell density. All loaded knees had significantly increased cell death rates and Mankin Scores compared to the non-loaded joints. Cartilage thicknesses did not systematically differ between loaded and control joints. Chondrocyte death and Mankin Scores were significantly increased in the loaded joints, thereby linking muscular exercise of physiologic magnitude but excessive intensity to cartilage degeneration and cell death in the rabbit knee."
couldn't get full study. Don't know why this was found to be catabolic.
In Vivo Dynamic Deformation of Articular Cartilage in Intact Joints Loaded by Controlled Muscular Contractions
In Vivo Dynamic Deformation of Articular Cartilage in Intact Joints Loaded by Controlled Muscular Contractions
"Cartilage deformation is known to cause deformations of the chondrocytes and their nuclei, and these deformations, in turn, are known to affect the biological signaling response of chondrocytes that control the maintenance and adaptation of the tissue"
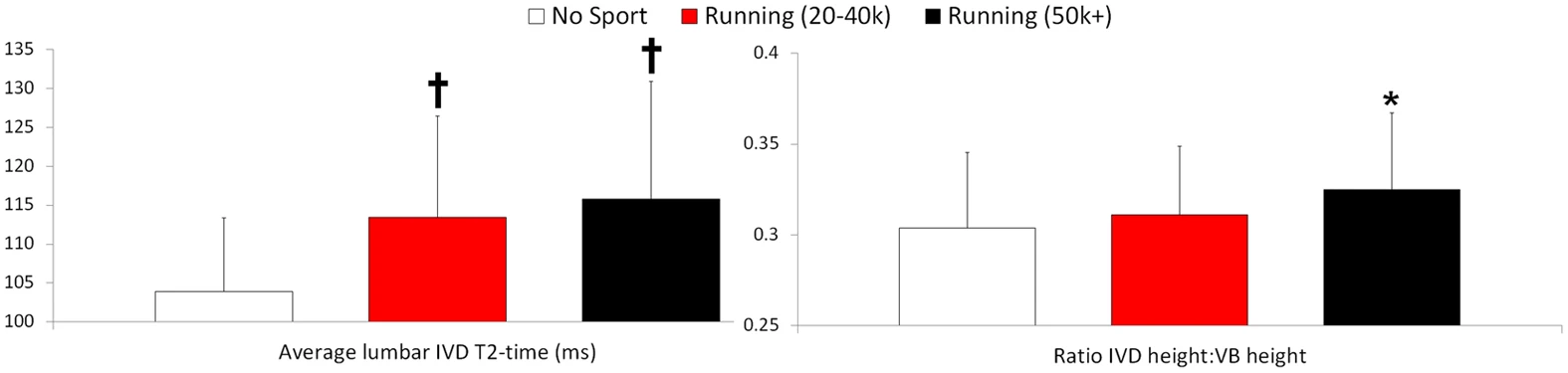
This is pretty significant. "Higher T2-times indicate better IVD hydration and glycosaminoglycan content."
No comments:
Post a Comment